|
CHEST TUBES; CHEST DRAINAGE The lungs are surrounded by a membrane or tissue called the "pleural membrane". Between the lung and this membrane is a space called the "pleural space". The pressure inside this space is normally negative. Air moves into the lung through a series of tubes or pathways, until the air reaches the end of the pathway. The pathway ends in a grape-like cluster of small air-filled sacs called alveoli (Image 1). These alveoli must remain open during inspiration (breathing in) and expiration (breathing out). In order for them to remain open and allow gases to move between the alveoli and blood vessels of the lung, the pressure outside the lung must remain lower than the pressure in the alveoli. A tear in the pleural membrane can allow air to enter into the pleural space. An accumulation of air within the pleural space will increase the pleural space pressure. If the pleural space pressure becomes higher than the pressure inside the lung, surrounding alveoli will collapse and air will be unable to enter this area of the lung. Air in the pleural space is called a "Pneuothorax". "Pneumo" means air and "thorax" means chest. The larger the area of collapse, the more serious the breathing problems (Image 2). Air can enter the pleural space if the lungs are diseased and the alveoli become susceptible to tearing. Mechanical ventilation can increase the risk for tearing because the breaths are delivered under pressure. Sometimes air can enter the lung when a central line is inserted. Trauma or surgery to the chest can also cause air to enter the plueral space and lead to pneumothorax. Blood can also collect in the pleural space and cause the pleural space pressure to rise. This is called a Hemothorax ("hemo" means blood). Blood and air can both enter the pleural space, especially following trauma or chest surgery. This is called a Hemopneumothorax. Sometimes a pneumothorax or hemothorax are described as a "Tension Pneumothorax" or "Tension Hemothorax". Tension is a word used to desribe pressure. A tension pneumo or hemothorax is "building presure". It is a term that is used to describe a rapidly expanding collection of air or blood. As the air or fluid expands, larger and larger areas of lung will collapse. Eventually, an entire lung can collapse and the air or blood can begin to "shift" or take up space around the opposite lung. As the expansion continues, the presure can compress the heart and blood vessels and lead to cardiovascular failure. A tension pneumothorax is very serious life-threatening event. The treatment for a pneumothorax or hemothorax is chest drainage. Chest drainage is accomplished by inserting a tube (called a Chest Tube), into the pleural space outside the lung. The tube is connected to a special drainage collection chamber called a Chest Drainage Unit. Fluid and air are removed and the pleural space pressure is reduced to normal. This allows the lung to reinflate. The Chest Drainage unit is designed to maintain a special seal that prevents any new air from entering the pleural space. If a tube was simply inserted in the space around the lung, air would be drawn into the tube each the patient inhaled, making the pneumothorax larger. To prevent this from happening, the end of the drainage system is placed "under water". This is called an "underwater seal". The undewater seal is analogous to a drinking straw submerged in water. Place a drinking straw into a glass of water. When you suck on the straw, you are breathing in through the straw. Because the straw is underwater, air does not enter the straw. Instead, the fluid rises into your mouth. If you blow air out through the straw, the escaping air will create bubbles in your glass. A chest drainage system uses the same principle. If we insert the end of a chest tube "under water", the "water seal" prevents any air from being drawn into the chest tube when the patient takes a breath. We can tell that the tube is in the space around the lung because the pressure changes will cause the fluid to rise up and down in the water seal chamber (like the straw). If the patient has air in the pleural space (pneumothorax), the air will exit the tube and escape through the underwater seal. If we see bubbles in the underwater seal, we know that the patient still has air in their pleural space. If we want to remove air (or fluid) even faster, we can connect the drainage system to a vacuum (called "suction"). Fluid will collect in a special chamber so we can monitor the amount of fluid that has been removed. Critically ill patients often have a lot of swelling or edema. Edema is produced when the water portion of the blood (called plasma) is forced into the tissues. For many reasons during critical illness, some of this fluid can also move into the pleural space.Plasma like fluid that leaks into the pleural space is called a Pleural Effusion. A large pleural effusion can also cause areas of the lung to collapse. A chest tube can be inserted into the pleural space to drain a pleural effusion. The problem with a pleural effusion is that insertion of a chest drainage tube does not eliminate the cause for the fluid leak. In fact, putting a tube into the pleural space can lower the pressure and encourage more pleural fluid to be produced. Pleural effusions are often just "watched". If the patient begins to develop signficant respiratory difficulty because of this fluid, we will drain the fluid off. Sometimes we drain the fluid intermittently. An intermittent or "one time" collection of fluid is sometimes called "tapping the lung". |
Image 1: Alveoli are the air filled sacs at the end of the air passages of the lung. |
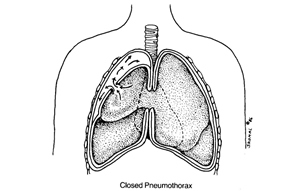
Image 2: Air in the pleural space causing an area of lung to collapse. |
|
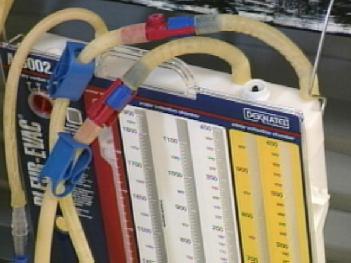
Image 2: Chest drainage unit. |
|
|
|
|
|
|
Last Reviewed: October 23, 2014


